What is adamantinoma?
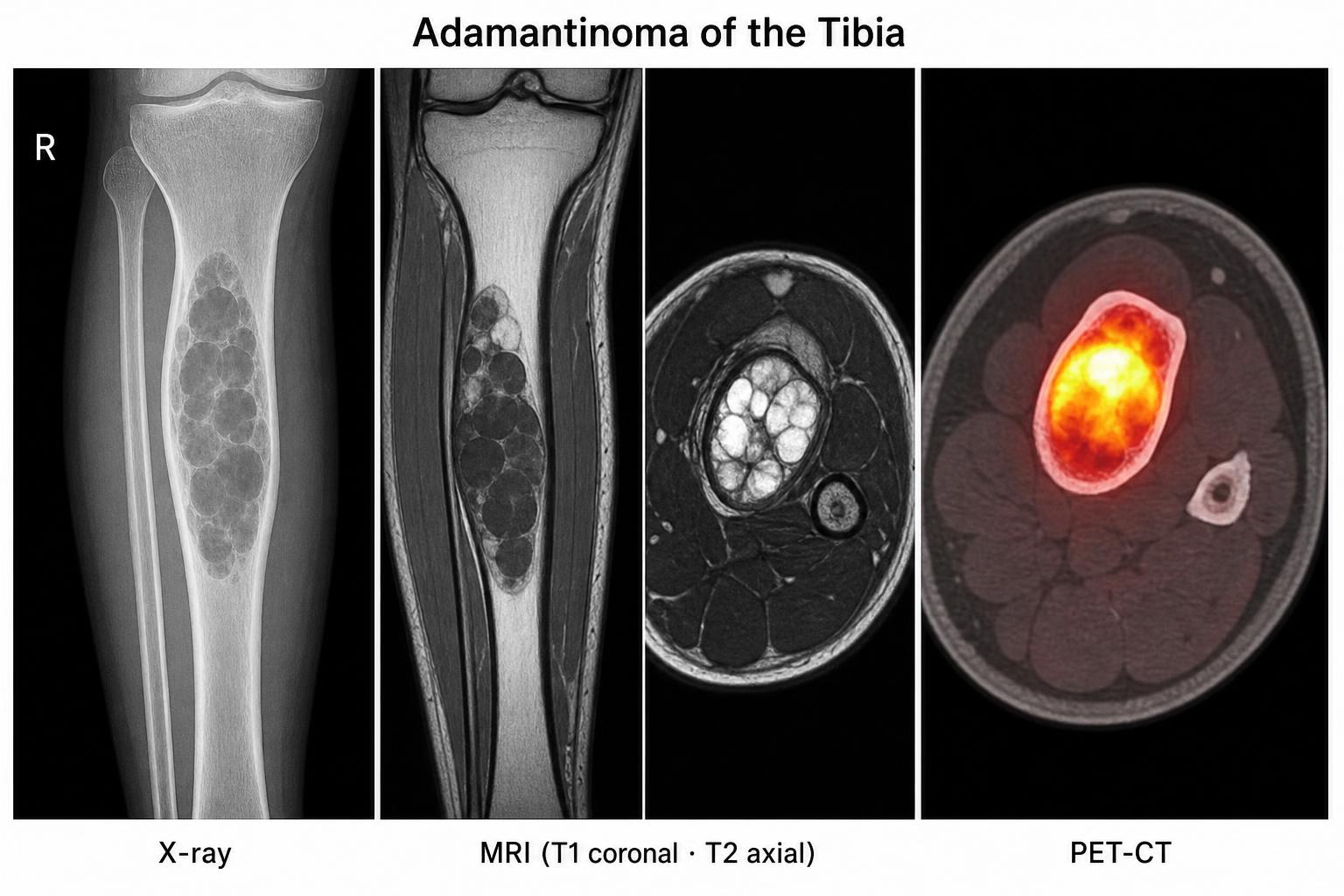
Adamantinoma is a rare bone tumour that originates from epithelial cells set within a fibrous bone background. It grows slowly but is locally aggressive and can recur many years after the original surgery. Distant spread is uncommon but possible — most often to the lungs.
Key point: A rare low-grade bone cancer where complete surgical removal is the cornerstone of cure.