Case 1 — Proximal femur chondrosarcoma
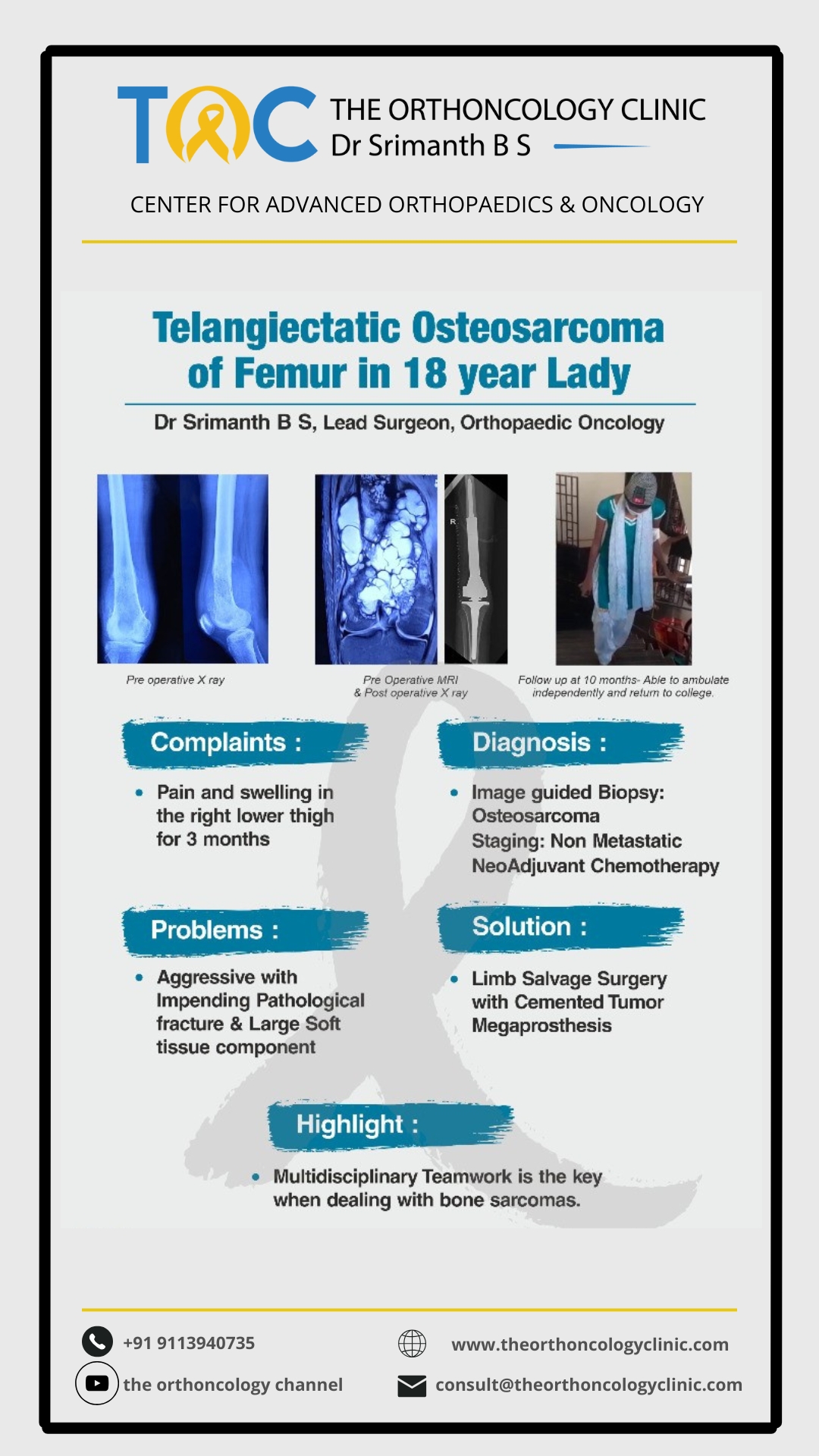
Limb salvage with tumour megaprosthesis reconstruction.
Limb salvage surgery removes cancerous bone or soft tissue in the arms or legs while preserving limb function. Advances in chemotherapy, radiotherapy, imaging and reconstructive implants have transformed care — from routine amputation to limb preservation in ≈95% of cases.
Complete tumour removal with healthy margins — local control rates above 95%.
Reconstruction restores joint motion, weight bearing and independence.
Patients retain self-image and return to daily activities and work.
The decision is made together — by you, your family and a sarcoma team — once we have the imaging, biopsy and response to neoadjuvant therapy in front of us.
Every step is planned by a multidisciplinary team — so the surgical decision is the best one for your tumour and your life.
X-rays, MRI, CT chest and PET-CT / bone scan for staging.
Image-guided core needle or open biopsy by the treating surgeon.
Tumour board with medical, radiation oncology, pathology and reconstruction.
Chemotherapy ± radiotherapy to shrink tumour and improve margins.
Reconstruction options, expected function and rehabilitation plan.
Three short case walkthroughs showing how planning, surgery and rehabilitation come together in everyday practice.
Limb salvage with tumour megaprosthesis reconstruction.
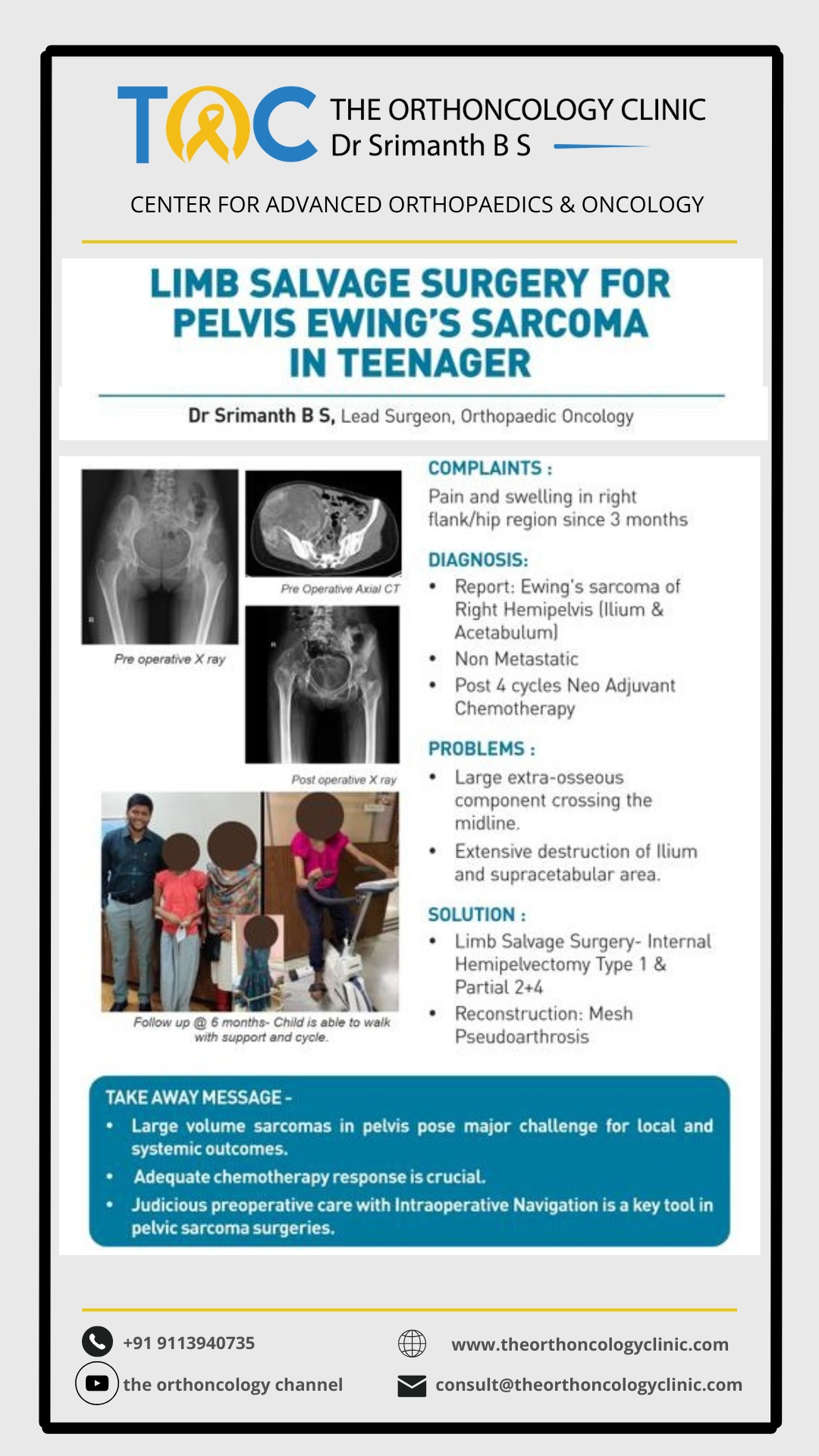
Limb-sparing internal hemipelvectomy and return to activity.
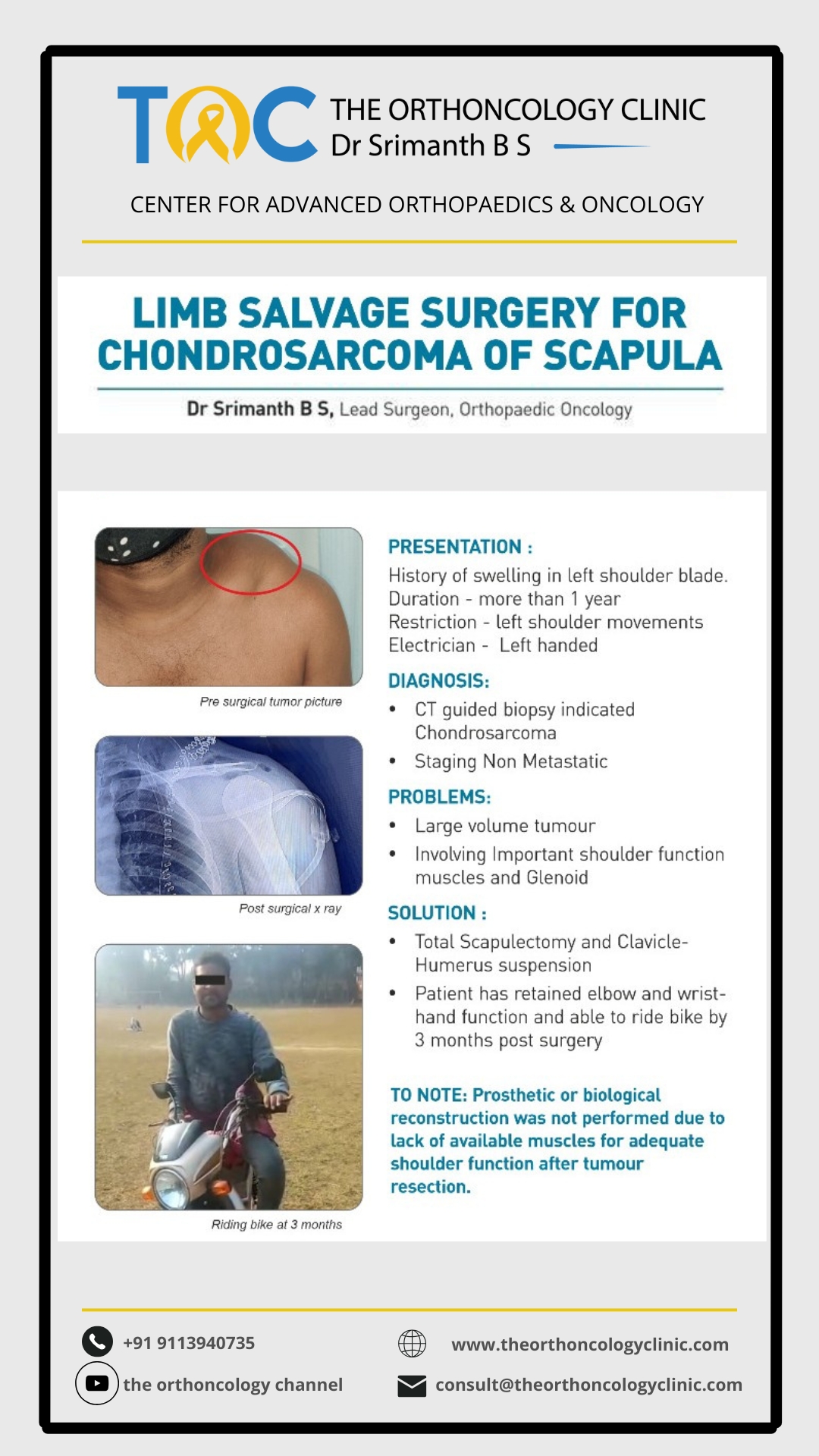
Limb-saving surgery with wrist fusion and ulna translocation.
Curated case posters showing diagnosis, surgical plan and recovery — published from The OrthOncology Clinic.
Decision factors include tumour location, age and growth potential, functional needs, cosmetic considerations, bone stock and soft-tissue envelope.
Large metallic implants restore bone and joint segments after resection — including expandable implants for children and 3D-printed custom designs.
Autograft, allograft, recycled tumour bone and 3D-printed solutions that promote natural healing and avoid long-term implant wear.
Composite reconstructions combined with patient-specific instrumentation, 3D printing, surgical navigation and augmented reality.
A durable, biologic limb-salvage option for children and young adults — the ankle is rotated to function as a knee, giving lifelong high-level function.
All major surgery carries risk. With sarcoma expertise these are minimised and actively managed.
Limb salvage surgery offers oncologically safe tumour removal with function-preserving reconstruction for most patients with limb sarcomas. Personalised planning by a multidisciplinary team — combined with advances in implants and biological techniques — delivers excellent survival and quality-of-life outcomes.
Book an Appointment